High-performance veterinary and human orthopedic surgical products certified to global medical standards.








Established in 2016, Medispirex operates a state-of-the-art manufacturing facility spanning 18,600㎡. We merge advanced biomechanical engineering with smart clinical integration to produce Class-III surgical implants. Over the last 12 years, our core technical group has pioneered surgical fixation advancements for trauma, spinal pathologies, and joint reconstruction.
A deep clinical and technical review of modern intramedullary osteosynthesis, material configurations, and design advancements.
Tibial shaft fractures represent one of the most common long-bone trauma presentation profiles in emergency orthopedic surgical departments worldwide. Over the past three decades, the management of these unstable extra-articular and simple intra-articular fractures has transitioned decisively toward closed reduction and internal fixation utilizing intramedullary nails (IMNs). Unlike traditional open plate fixation, which disrupts the periosteal blood supply and requires extensive soft-tissue dissection, intramedullary nails serve as load-sharing internal splints. This biological fixation preserves the surrounding envelope, optimizes blood flow to the fracture site, and promotes rapid endosteal callus formation.
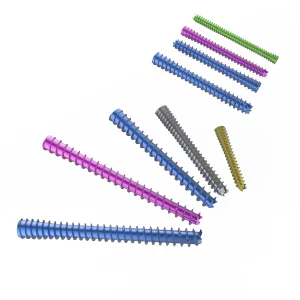
Modern implant engineering focuses heavily on resolving historical clinical pain points. Early IM nail designs frequently suffered from rotational instability, distal screw backing-out, and localized patellofemoral pain. Through multi-planar locking configurations, proximal dynamic slot variations, and anatomically curved profiles, contemporary manufacturers have reduced post-operative complications by over 40%. The incorporation of distal multi-planar locking options ensures that even distal metaphysis fractures can be stabilized effectively, expanding the indications of intramedullary nailing closer to the joint line.
Comparing entry pathways and their biomechanical impacts on patient recovery and surgeon workflow.
One of the major discussions in modern trauma orthopedics is the choice of surgical approach for tibial nailing. The traditional infrapatellar approach requires hyperflexing the knee (typically >90°), which can induce significant mechanical displacement of proximal bone fragments during reaming. It is also associated with high rates of chronic anterior knee pain (up to 50-70% in some clinical series) caused by patellar tendon disruption or infrapatellar branch damage of the saphenous nerve.
Conversely, the suprapatellar insertion technique utilizes a semi-extended knee position (15° to 30° flexion). This trajectory allows the quadriceps muscle to remain relaxed, eliminating deforming forces and maintaining bone alignment. A dedicated protective sleeve system is inserted through the quadriceps tendon to shield the patellofemoral cartilage from mechanical wear during reaming and nail positioning. Medispirex, through its extensive clinical OEM partnerships, has developed advanced suprapatellar instrumentation sets that offer surgeons precise guide wire targeting while minimizing intraoperative fluoroscopy exposure.
| Feature Parameter | Suprapatellar Approach (Semi-Extended) | Infrapatellar Approach (Hyperflexed) |
|---|---|---|
| Knee Position during Insertion | 15° - 30° Flexion (Semi-Extended) | 90° - 120° Flexion (Hyperflexed) |
| Proximal Segment Control | Excellent; Quadriceps pull is eliminated | Poor; High risk of procurvatum deformity |
| Anterior Knee Pain Incident Rate | Significantly reduced (<15%) | High (30% - 70% clinically reported) |
| Cartilage Exposure Risks | Protected via inner cannula cannula sleeve | Low risk of direct contact but high soft tissue tension |
| Fluoroscopy Alignment Verification | Simplified AP and Lateral imaging in extension | Requires manual leg adjustment for lateral view |
As the medical device sector faces tightening regulatory oversight and hospital budgetary pressures, medical distributors are shifting focus toward manufacturing efficiency and supply chain visibility. Modern manufacturing in China has transitioned from simple labor-intensive production to high-precision Industry 4.0 smart factories.
Medispirex utilizes automated CNC machining centers, automated sandblasting systems, and advanced electrochemical anodizing lines. By integrating our enterprise resource planning (ERP) system directly with our quality management system, we track raw materials from the initial titanium alloy rod (ASTM F136 compliant) through to final sterile packaging. This level of traceability complies with both ISO 13485 standards and European Union MDR requirements, assuring global medical distributors of consistent product quality.
Furthermore, our industrial setup in the Yangtze River Delta offers access to a dense network of raw material processing plants, thermal treatment facilities, and sterilization houses. This proximity helps us maintain short lead times (averaging 15 to 30 days) and competitive pricing compared to European or North American manufacturing sites.
Multi-axis Citizen CNC sliding-head lathes perform milling, drilling, and thread cutting in a single setup, guaranteeing concentricity tolerances within ±0.005mm.
Type II anodic oxidation creates a uniform titanium dioxide layer, which increases fatigue life and reduces cold welding of titanium locking screws.
Dynamic compression bending tests are performed according to ASTM F1264 guidelines, verifying that our nails can withstand over 1 million loading cycles without structural failure.
Inside our 18,600㎡ facility: a visual overview of our advanced orthopedic implant manufacturing lines.













Understanding the engineering behind Ti-6Al-4V ELI (ASTM F136) and its biomechanical benefits.
The choice of raw material directly impacts the fatigue performance and biocompatibility of tibial implants. Medispirex manufactures intramedullary nails using medical-grade Ti-6Al-4V ELI (Extra Low Interstitial) titanium alloy, adhering to ASTM F136 and ISO 5832-3 standards. Titanium is preferred over traditional 316L stainless steel for several reasons:
First, its elastic modulus (approx. 110 GPa) is closer to that of cortical bone (approx. 10–30 GPa) than stainless steel (approx. 200 GPa). This reduce the effects of stress shielding—a phenomenon where the stiffness of an implant prevents physiological loads from transferring to the bone, potentially leading to bone resorption and delayed healing. Second, titanium's passivation layer provides high corrosion resistance in the saline environment of human tissue, lowering the risk of metallosis or adverse immune responses.
Answers to technical and commercial questions for medical distributors, purchasing managers, and orthopedic surgeons.
A wider selection of bone fixation systems, locking screws, and surgical instrument setups.